This study contributes to the broader discourse on urban design for children, offering insights into how cities can create more inclusive, engaging, and health-promoting environments. It supports and adds to existing literature, finding that the alignment of play initiatives with public health goals, and strong collaboration between local government departments are effective in supporting children’s play on the strategic level. It identifies barriers to play in policy, namely budget constraints and deprioritisation of play.
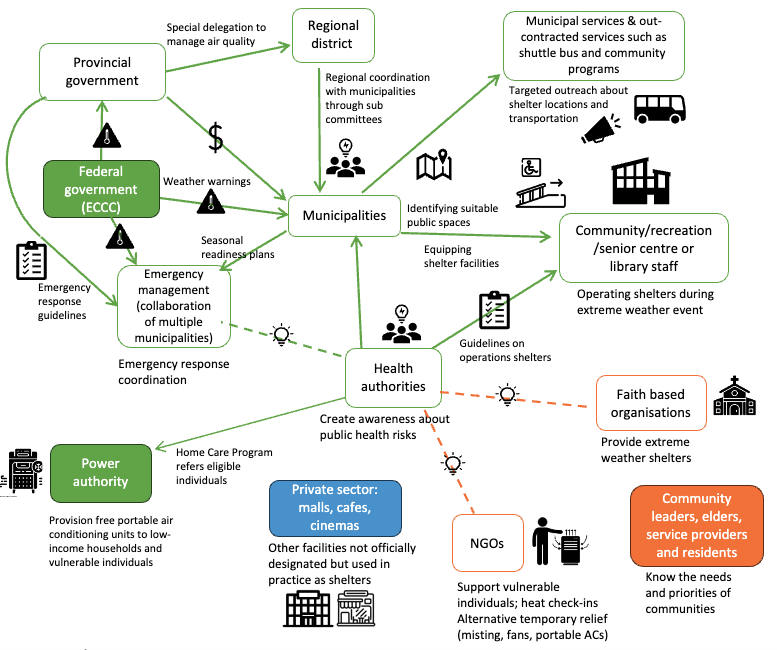
Extreme heat and wildfire smoke are a growing concern in cities. Cooling and cleaner air centres can provide a much-needed respite but too often they’re set up reactively and inconsistently. Our study explores what works, what doesn’t, and how cities can design these spaces to be reliable, inclusive, and accessible for all.

Are you prepared for the health risks of extreme heat? Our new study shows that exposure to extreme heat increases the risk of mortality from Non-Communicable Diseases. Check out our systematic review of the effects of extreme heat, both indoors and outdoors, on health in the UK.